



New CMS 1500 Claim Forms - HCFA (Version 02/12) 25
₹8160 -35% ₹5300/-
NextDayLabels - CMS 1500 / HCFA 1500 Insurance Cla
₹6720 -36% ₹4300/-
NextDayLabels - CMS 1500 / HCFA 1500 Insurance Cla
₹12500 -40% ₹7500/-

New CMS 1500 Health Insurance Claim Forms, HCFA Ap
₹7820 -36% ₹5000/-
NextDayLabels - CMS 1500 / HCFA 1500 Insurance Cla
₹23390 -38% ₹14500/-

NextDayLabels - UB-04 (CMS 1450) Health Hospital I
₹11720 -36% ₹7500/-
UB-04 (CMS 1450) Health Hospital Insurance Claim F
₹6150 -30% ₹4300/-

UB-04 (CMS 1450) Health Insurance Claim Form (Pack
₹10900 -33% ₹7300/-

NextDayLabels - ADA Dental Claim Insurance Claim F
₹13390 -35% ₹8700/-

New CMS 1500 Claim Forms - HCFA (Version 02/12) (2
₹8000 -35% ₹5200/-

Compuchecks New Cms 1500 Claim Forms - Hcfa (Versi
₹9700 -35% ₹6300/-

500 CMS 1500 Claim Forms, Current HCFA 02/2012 New
₹10940 -36% ₹7000/-
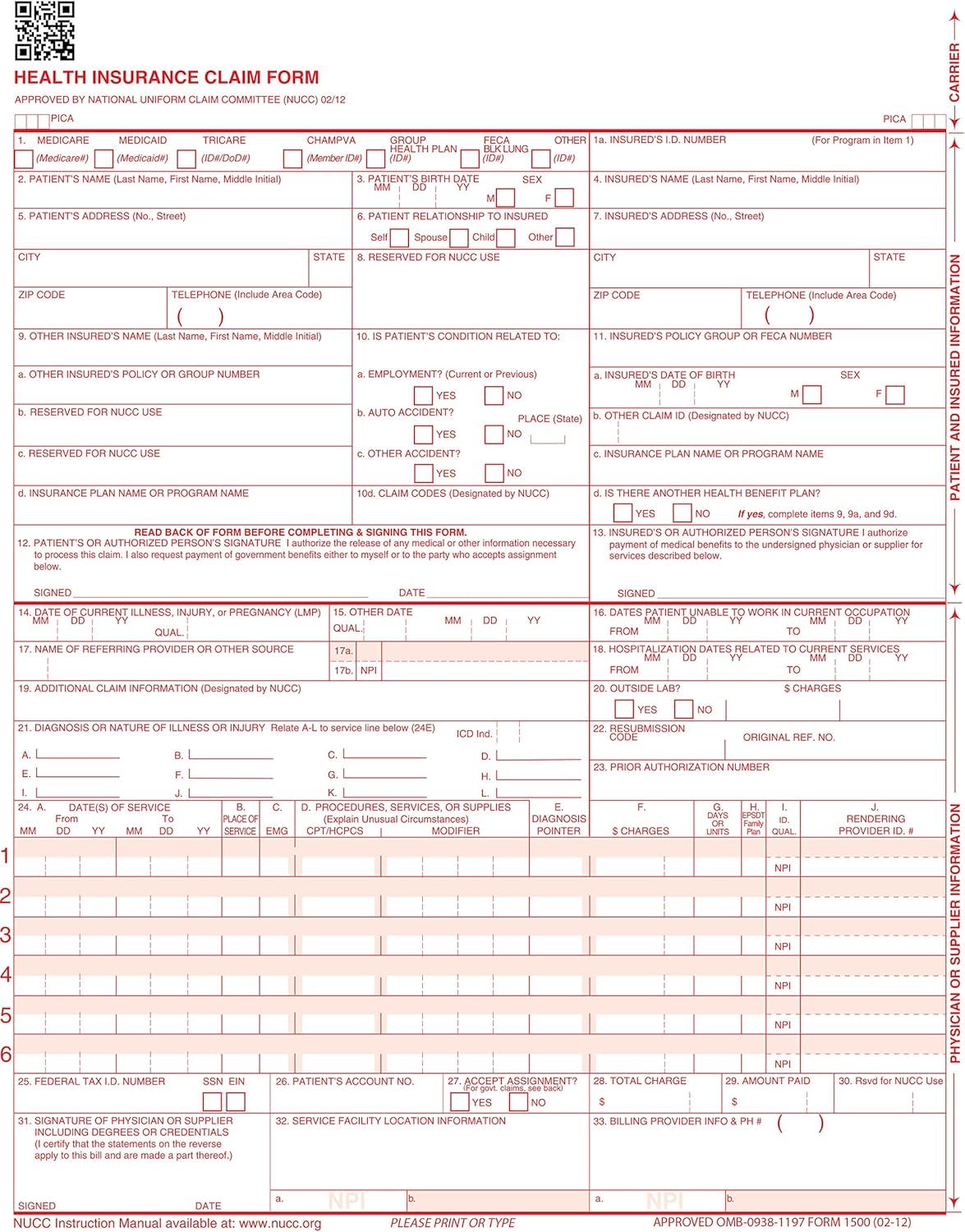
CMS 1500 Claim Forms "ICD-10" HCFA (Version 02/12)
₹27750 -38% ₹17200/-

Facial Intake, Consent & Aftercare Forms | 75 Pack
₹8070 -38% ₹5000/-

Lashicorn Covid-19 Release of Liability Forms | 50
₹6370 -34% ₹4200/-
Botox Intake, Consent, and Aftercare Form | 75 Pac
₹7250 -31% ₹5000/-

NEW CMS 1500 Claim Forms - HCFA (Version 02/12) 10
₹6670 -31% ₹4600/-

New CMS 1500 Claim Forms - 25 Sheets (02/12 Versio
₹6400 -39% ₹3900/-

Health Insurance Claim Forms, New CMS-1500, HCFA (
₹7670 -40% ₹4600/-
New CMS 1500 Health Insurance Claim Forms, HCFA Ap
₹8690 -39% ₹5300/-
New CMS 1500 Health Insurance Claim Forms, HCFA Ap
₹6720 -33% ₹4500/-

UB-04 (CMS-1450) Health Hospital Insurance Claim F
₹8010 -30% ₹5600/-

New CMS 1500 Health Insurance Claim Forms, HCFA Ap
₹18440 -36% ₹11800/-

Maintenance Request Forms on 3 Part Carbonless Pap
₹16170 -40% ₹9700/-

DOT Medical Examination Report Forms MCSA-5875, (1
₹16840 -40% ₹10100/-